
The pharmacotherapy arms race for diabetes and obesity has gone to the next level.
Is more always better?
Glucagon-like peptide 1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) receptor agonists have become incredibly popular treatment options for people with diabetes and/or obesity due to their effectiveness at improving glycaemic control and weight reduction – as well as a whole bunch of other medical conditions – in recent years.
Pharmaceutical companies have since developed dual GIP and GLP-1 receptor agonists to expand the potential number of receptors and pathways they can target with a single drug to one-up their rivals.
It’s therefore not surprising to come across the results of the first phase 3 trial of a triple hormone receptor agonist named retatrutide, which also targets glucagon receptors in addition to GIP and GLP-1 receptors.
“The results of the TRANSCEND-T2D-1 clinical trial suggest that once-weekly retatrutide could offer first-line treatment for early type 2 diabetes without background antihyperglycaemic medication, providing effective glycaemic control in addition to [the] benefits of clinically relevant weight reduction and improvement in cardiometabolic parameters with no severe hypoglycaemia events reported in the study, as well as gastrointestinal side-effects and an adverse event profile consistent with other therapies with GLP-1 agonist activity,” the authors of the new trial wrote in The Lancet.
Researchers recruited 537 adults (aged ≥18 years) with type 2 diabetes, a BMI of ≥23.0kg/m2, and a HbA1c that sat between 7.0% and 9.5% despite diet and exercise, from 48 research institutes and hospitals across India, Mexico, and the USA.
Recruited participants were naïve to insulin therapy (excluding its use for gestational diabetes or up to 14 days of acute treatment) and had not used antihyperglycaemic medications in the past 90 days. Participants who had experienced severe hypo- or hyperglycaemia in the past six month were excluded.
The recruited patients had a mean age of 48.8 years, HbA1c concentration of 7.9%, weight of 96.9kg, and BMI of 35.8kg/m2 at baseline. Most participants were female (55%) and 85% of participants had never previously used antihyperglycaemic medication. The average duration of type 2 diabetes was 2.5 years.
Patients received either 4mg, 9mg, or 12mg of retatrutide or placebo, administered via weekly subcutaneous injections. All patients receiving retatrutide started with a 2mg dose but increased the administered amount every four weeks until the assigned dose was reached. The study design involved a four-week screening period, a 40-week treatment period, and a four-week follow-up period.
Of the 537 adults recruited for the study, 134 were randomised to 4mg of retatrutide, 133 to 9mg, 136 to 12mg, and 134 to placebo. There were 37 participants who discontinued the active treatment and 10 participants who discontinued the placebo during the study. Participants in the 9mg and 12mg retatrutide group cited adverse events as the most common reason for discontinuing the study, whereas participants in the 4mg retatrutide group and the placebo group tended to withdraw themselves from the study.
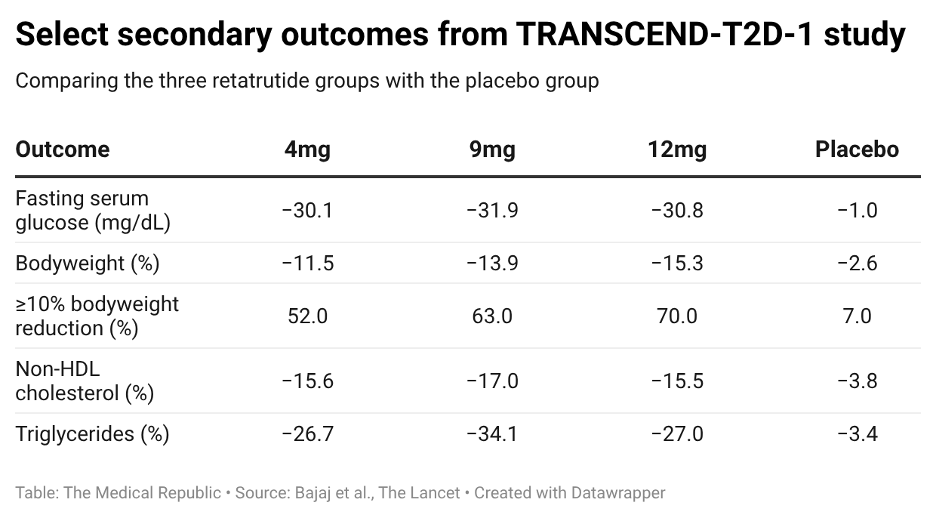
The study met its primary endpoint, with retatrutide showing a greater reduction in HbA1c between baseline and 40 weeks (i.e., the end of the treatment period) than placebo. The average change in HbA1c was -1.69% for the 4mg retatrutide group, -1.86% for the 9mg group, and -1.94% for the 12mg group compared to -0.81% for the placebo group. Several key secondary outcomes were also met, including the change in fasting serum glucose, bodyweight, and non-HDL cholesterol.
The researchers felt that the improvements in glycaemia confirmed the benefits of targeting GIP, GLP-1, and glucagon receptors in parallel, and that the addition of GIP co-agonism could potentially reduce HbA1c levels towards near-normoglycaemic levels.
“Although dual GIP and GLP-1 receptor agonism has been shown to improve glycaemic control by enhancing glucose-dependent insulin secretion and suppressing glucagon secretion, delaying gastric emptying, and improving insulin sensitivity, additional research on the role of glucagon agonism in the setting of hyperglycaemia or normoglycaemia is warranted to further understand the role of glucagon agonism in glycaemic control,” they wrote.
“Retatrutide appears to preserve this degree of glycaemic lowering while producing meaningfully greater weight reduction, potentially attributable to the additional glucagon receptor activation, which might increase energy expenditure and fatty acid oxidation and impart an additive effect on lowering food intake.”
Assistant Professor Shuyao Zhang and Professor Ildiko Lingvay, a pair of endocrinologists from UT Southwestern Medical Centre in the United States who penned an accompanying commentary for the new research, stated that the results “are of restricted clinical use or scientific impact” because of the use of a placebo rather than an active control.
“In the absence of active comparator trials, indirect comparisons with similarly designed trials that enrolled treatment-naive participants with type 2 diabetes suggest that TRANSCEND-T2D-1 produced placebo-subtracted HbA1c reductions… broadly similar to those reported in SUSTAIN-1 with semaglutide 1·0 mg (–1·53%) and SURPASS-1 (–1·60%) suggesting a plateau effect on glycaemic control,” they wrote.
“In contrast, the placebo-subtracted weight reduction was greater compared with both SUSTAIN-1 (calculated at approximately –3·9% for 1 mg semaglutide) and SURPASS-1 (calculated at approximately –7·9% for 15 mg tirzepatide).
“Although indirect, these comparisons suggest a potential incremental benefit from added glucagon agonism on weight reduction, but not for glycaemic control.”
Treatment-emergent adverse events occurred at similar rates between the retatrutide groups and the placebo group: 63% for the 4mg group, 64% for the 9mg group, 63% in the 12mg group, and 57% in the placebo group. Diarrhoea, nausea, and vomiting were the most commonly occurring treatment-emergent adverse events, all occurring in at least 15% of patients in each of the retatrutide groups and in between 2% and 4% of patients in the placebo group. Fourteen participants experienced a serious adverse event: six in the 4mg group, one in the 9mg group, five in the 12mg group, and two in the placebo group.
A major limitation of the study was that it only recruited patients who were largely medication-naïve, thereby reducing the generalisability of the results to the wider cohort of people with type 2 diabetes who may already be on prescription medications for glycaemic control. Furthermore, the 40-week treatment period was potentially not long enough to allow for long-term safety and efficacy to be established, although studies with longer treatment periods are either planned or underway. The study was also conceived, designed, and supervised by Eli Lilly.
Despite their concerns regarding the interpretation of the results, Professors Zhang and Lingvay concluded that multi-agonist agents were an area to watch in the coming years.
“Retatrutide, the first triple-agonist agent, may not provide incremental improvements in glycaemic control compared with existing monoagonist and dual-agonist therapies, but its principal advantage is greater weight reduction. Whether this incremental weight loss translates into improved clinical outcomes, enhanced quality of life, or other patient-reported benefits remains unclear.
“GLP-1 receptor monoagonists have already shown benefits to weight, glycaemia, cardiovascular risk factors, cardiorenal outcomes, liver health, and some obesity-related complications such as osteoarthritis.
“As a plethora of multireceptor modulators are being developed, the question is not merely whether they will have the same benefits but whether broader receptor engagement confers distinct metabolic advantages (such as improvements in bone health or muscle strength), disease-modifying effects for either diabetes (such as β-cell preservation) or obesity (such as resetting the defended weight), and improved tolerability resulting from the additional mechanism(s) of action.
“For retatrutide and other multireceptor modulators to warrant a distinct role in treatment algorithms, they must show clinically meaningful benefits beyond what is already attributed to GLP-1 receptor agonism, with advantages that clearly outweigh any additional tolerability concerns or treatment burden.”
